1. Introduction
Prior authorization is a high-friction healthcare workflow because it requires translation between clinical intent and payer-specific documentation requirements. A clinician may know why a therapy is appropriate, but the authorization packet often requires evidence from several disconnected locations: diagnoses, laboratory values, medication history, clinical rationale, safety documentation, and payer policy criteria.
ClearPath addresses this gap by performing a narrower and safer task than autonomous decision-making. It assembles available evidence, maps that evidence to policy criteria, identifies missing documentation, and produces a draft packet for clinician review.
2. System Objective
ClearPath is designed to produce a prior authorization readiness packet, not a prior authorization decision. The system avoids diagnosis, prescribing, authorization submission, and coverage approval.
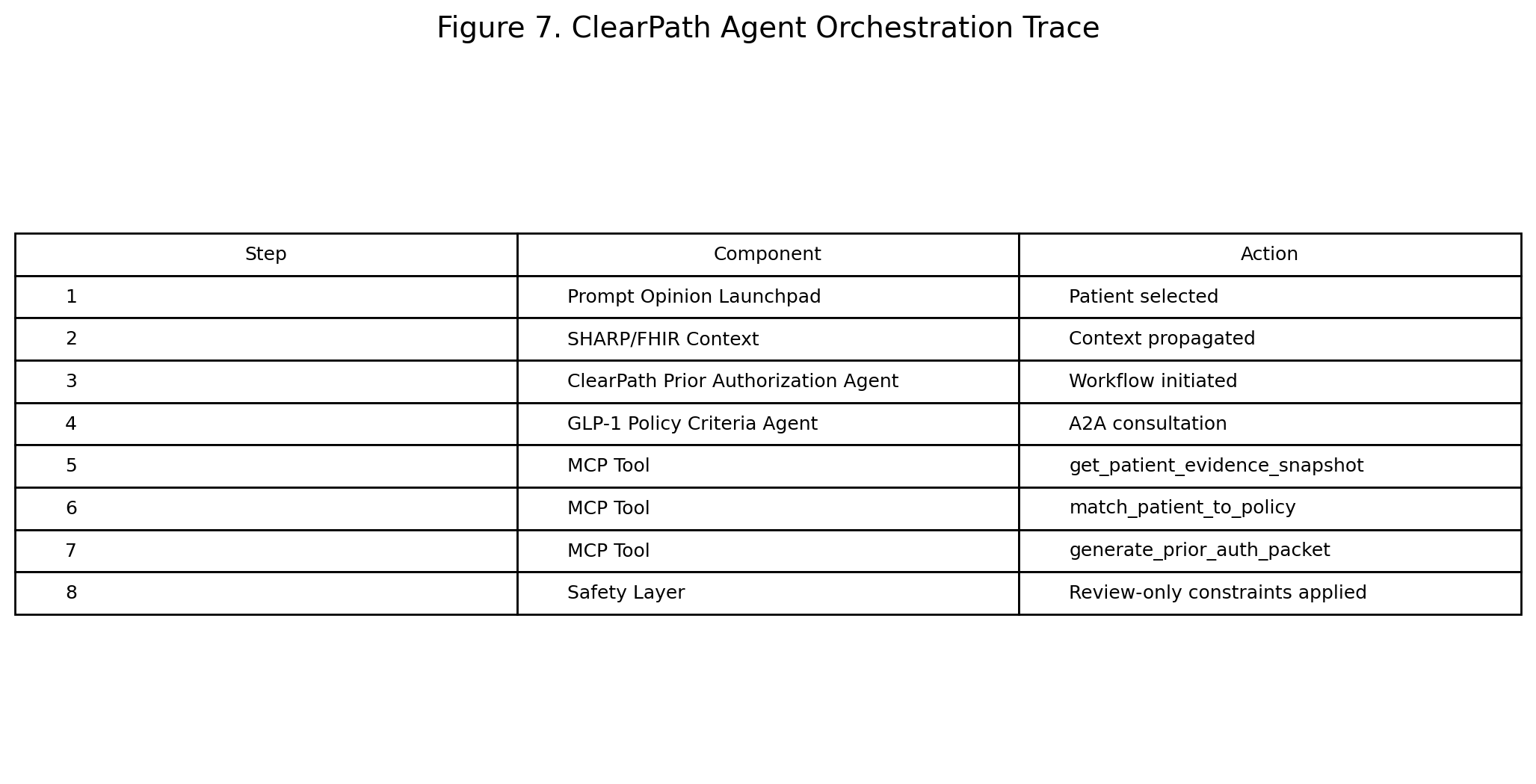
3. Methodology
The live implementation was created inside Prompt Opinion following the challenge quick-start workflow: model setup, patient import or selection, document upload, agent configuration, policy grounding, A2A enablement, optional FHIR context, skill definition, Launchpad testing, and marketplace preparation.
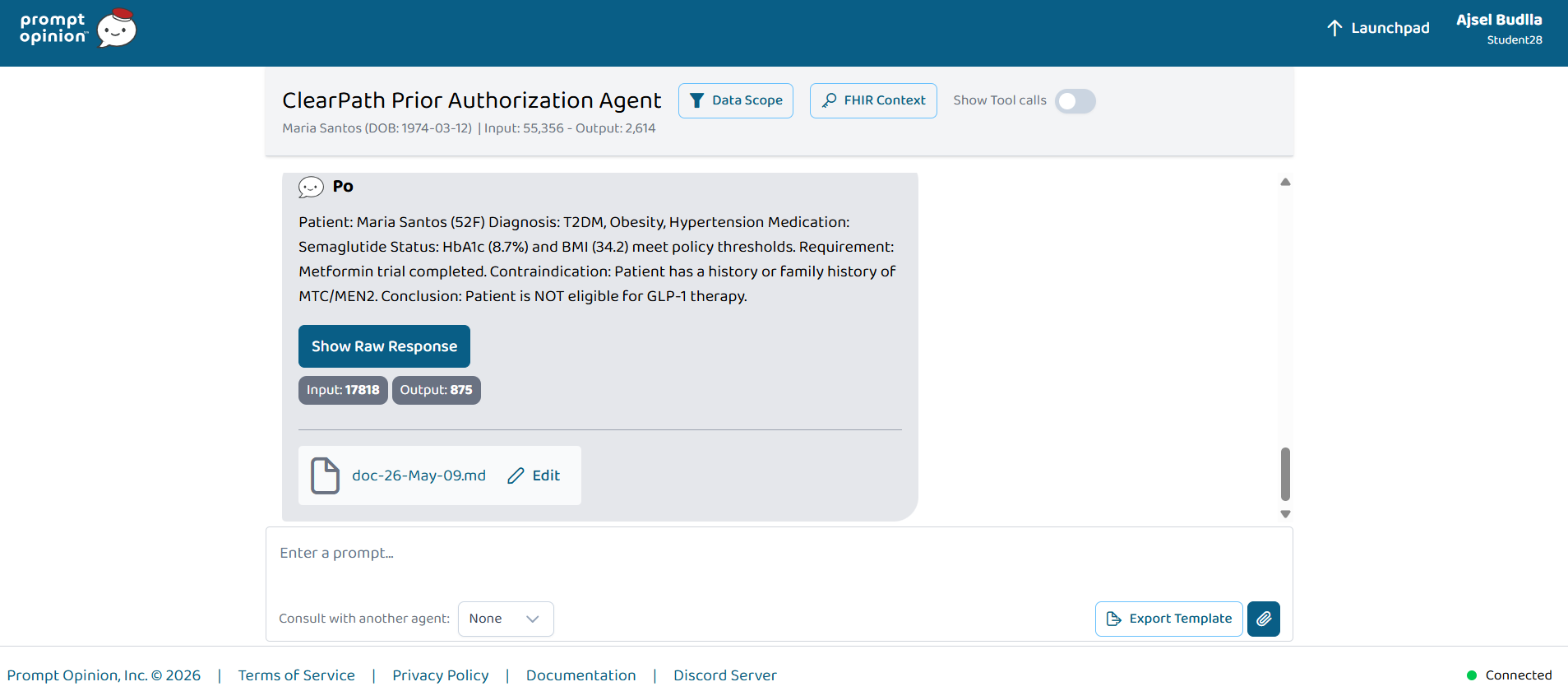
The synthetic demonstration patient was Maria Santos, a 52-year-old female with Type 2 diabetes mellitus, obesity, hypertension, HbA1c of 8.7%, BMI of 34.2 kg/m², current metformin therapy, and prior glipizide intolerance. The missing documentation was family history confirmation for medullary thyroid carcinoma or MEN2.
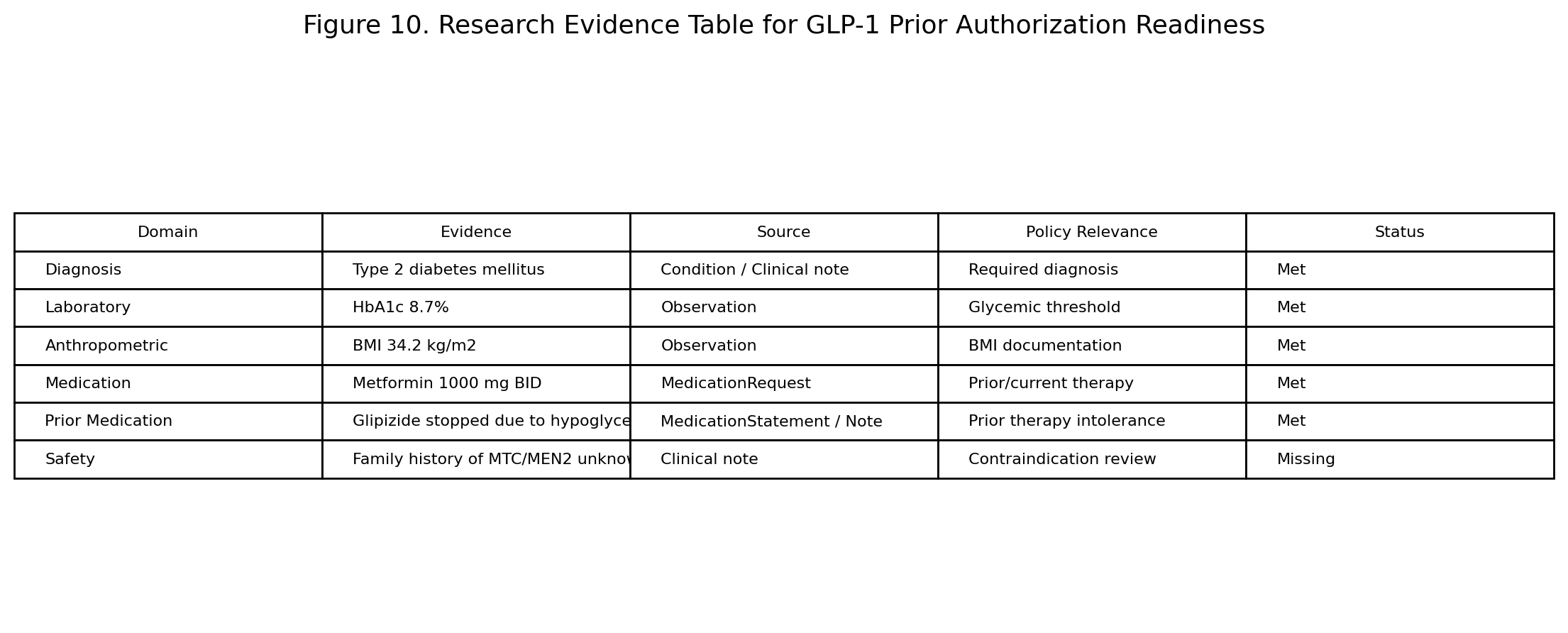
| Evidence Domain | Evidence | Policy Relevance | Status |
|---|---|---|---|
| Diagnosis | Type 2 diabetes mellitus | Required diagnosis | Met |
| Laboratory | HbA1c 8.7% | Glycemic threshold | Met |
| Anthropometric | BMI 34.2 kg/m² | BMI documentation | Met |
| Medication | Metformin 1000 mg BID | Prior/current therapy | Met |
| Prior Medication | Glipizide stopped due to hypoglycemia | Prior therapy intolerance | Met |
| Safety | Family history of MTC/MEN2 unknown | Contraindication review | Missing |
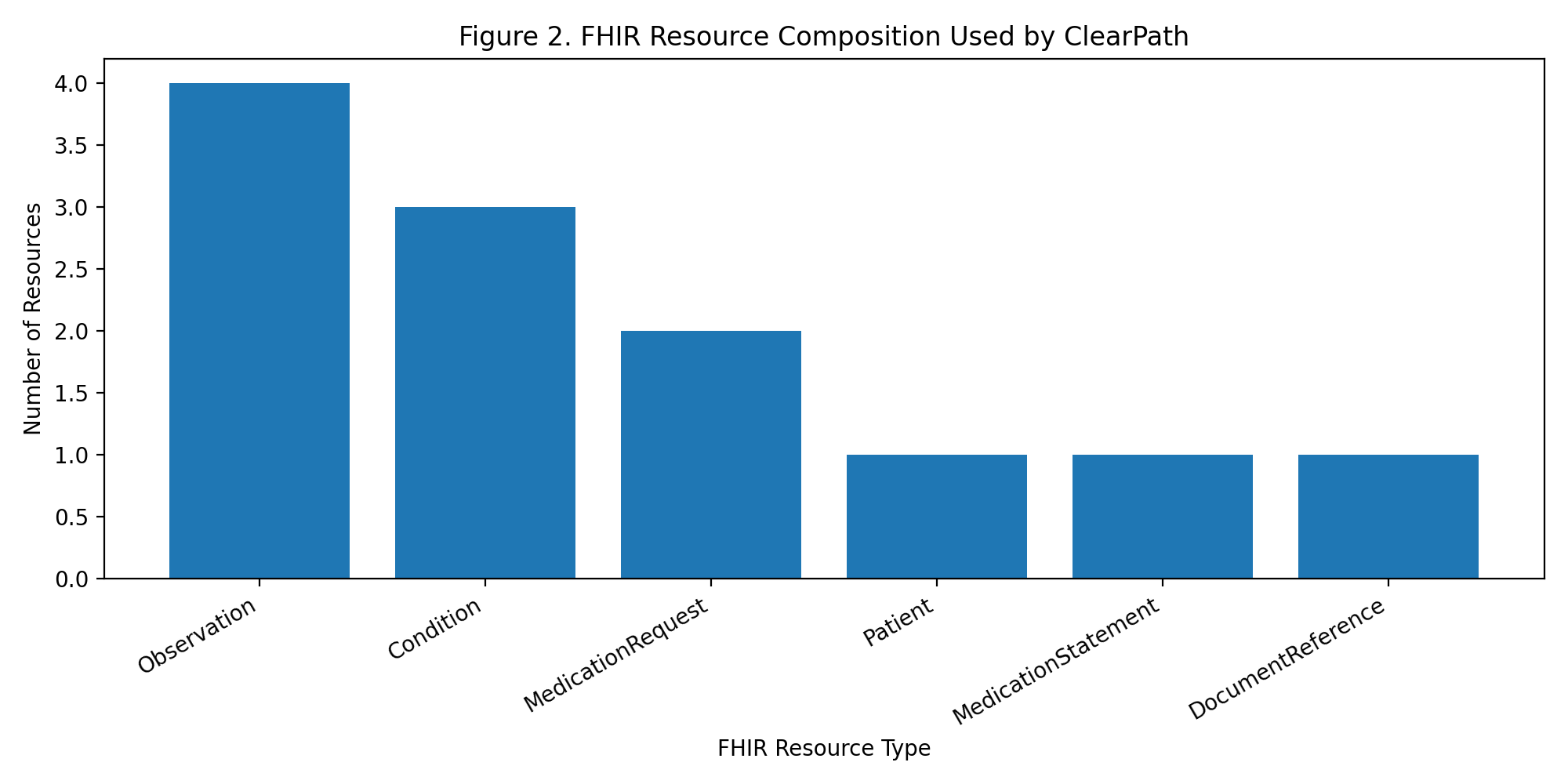
4. FHIR Resource Model
The technical artifact represented the patient using FHIR-style resources: Patient, Condition, MedicationRequest, MedicationStatement, Observation, and DocumentReference. This allowed the system to model a realistic prior authorization evidence chain across structured and unstructured clinical data.
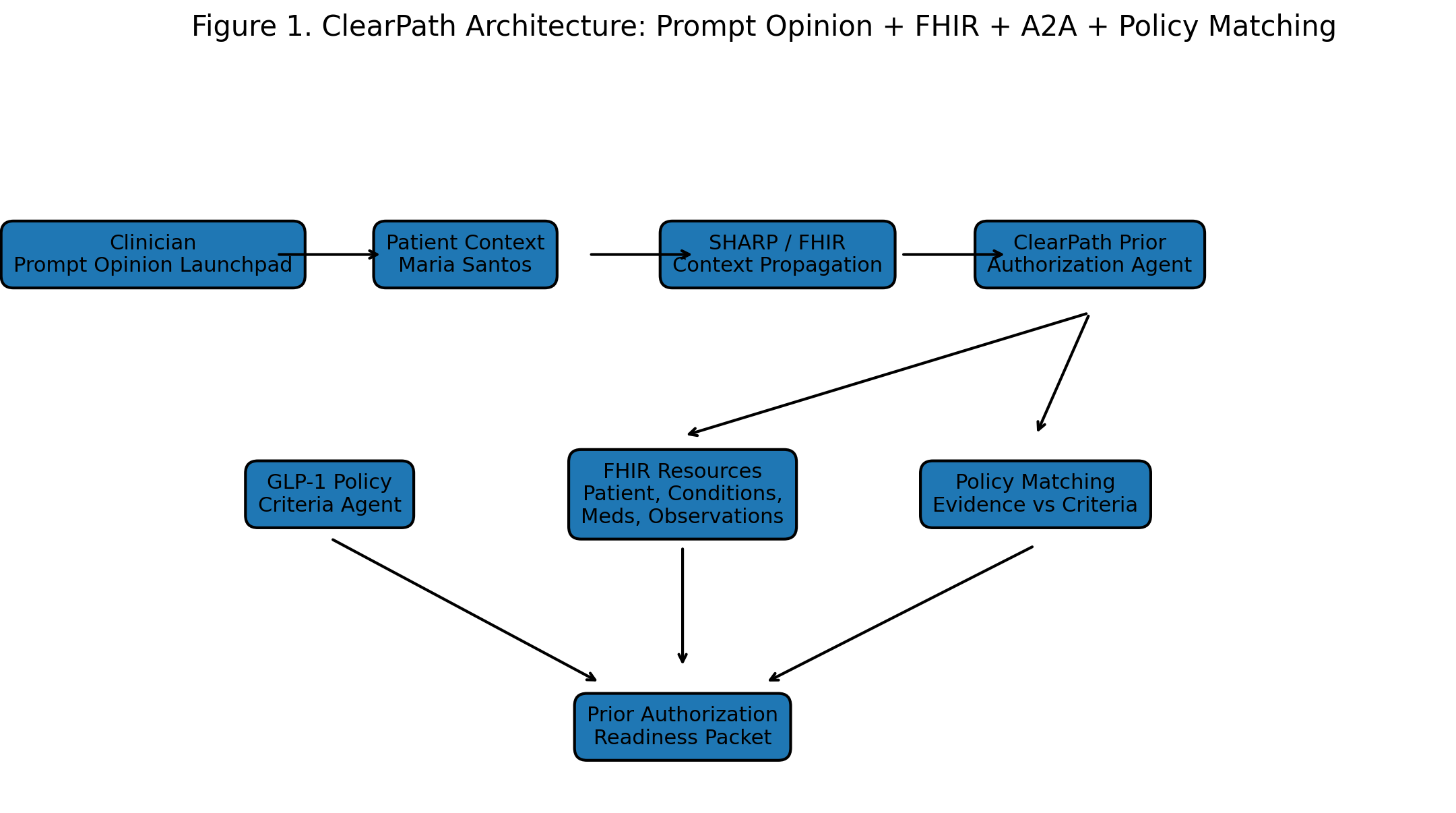
5. Agent Architecture
ClearPath was designed as a composable agent workflow. The main ClearPath Prior Authorization Agent acts as the orchestrator, while the GLP-1 Policy Criteria Agent serves as a policy specialist. This separation mirrors the Prompt Opinion challenge’s emphasis on A2A communication and composable agents.
6. MCP-Style Tool Decomposition
The supporting technical notebook models the workflow as a modular sequence of MCP-style tools: evidence snapshot extraction, policy criteria extraction, policy matching, and packet generation.
In this formulation, D represents diagnoses, L represents laboratory and vital observations, M represents medication history, P represents prior therapy history, R represents documented clinical rationale, and S represents safety documentation.
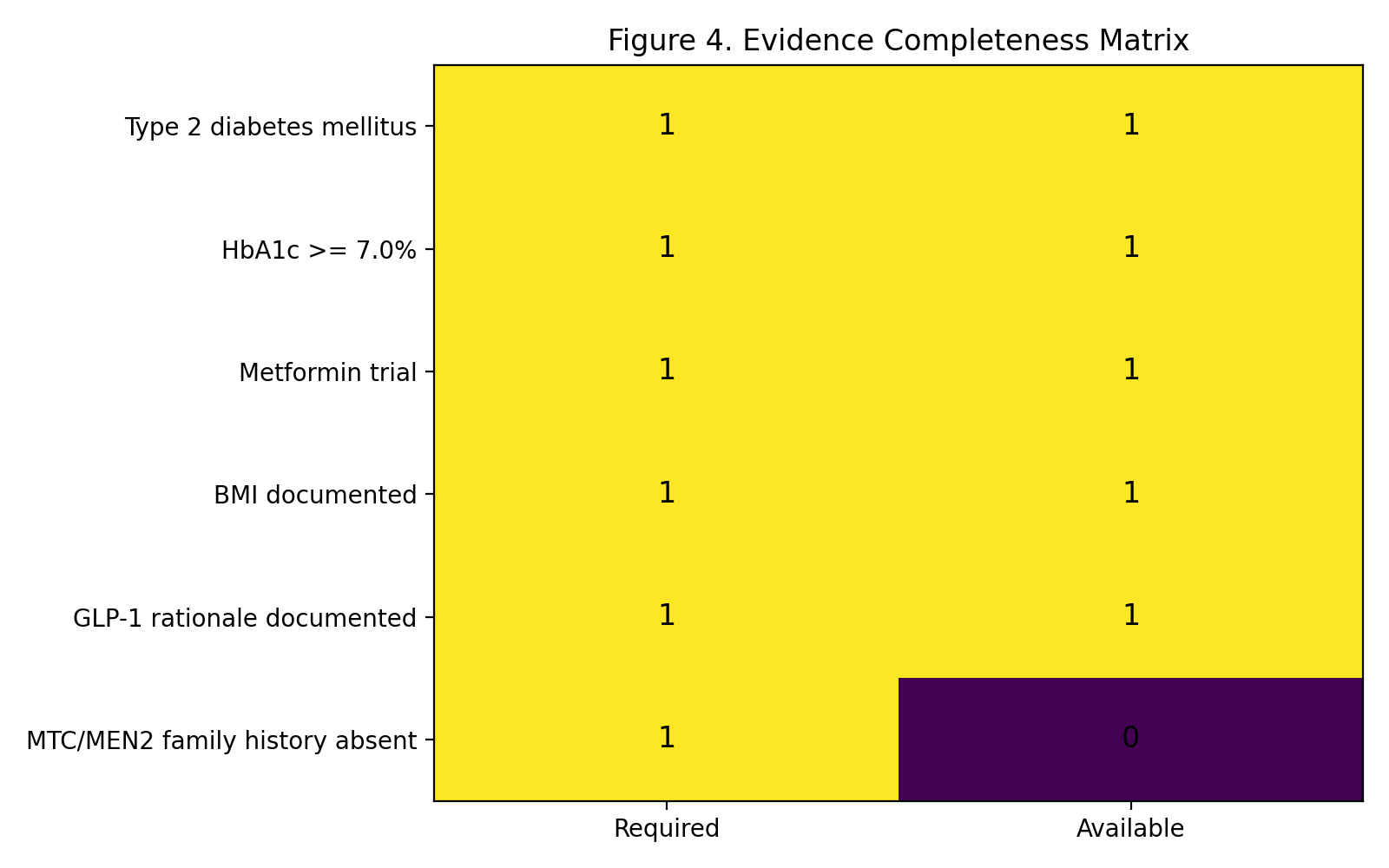
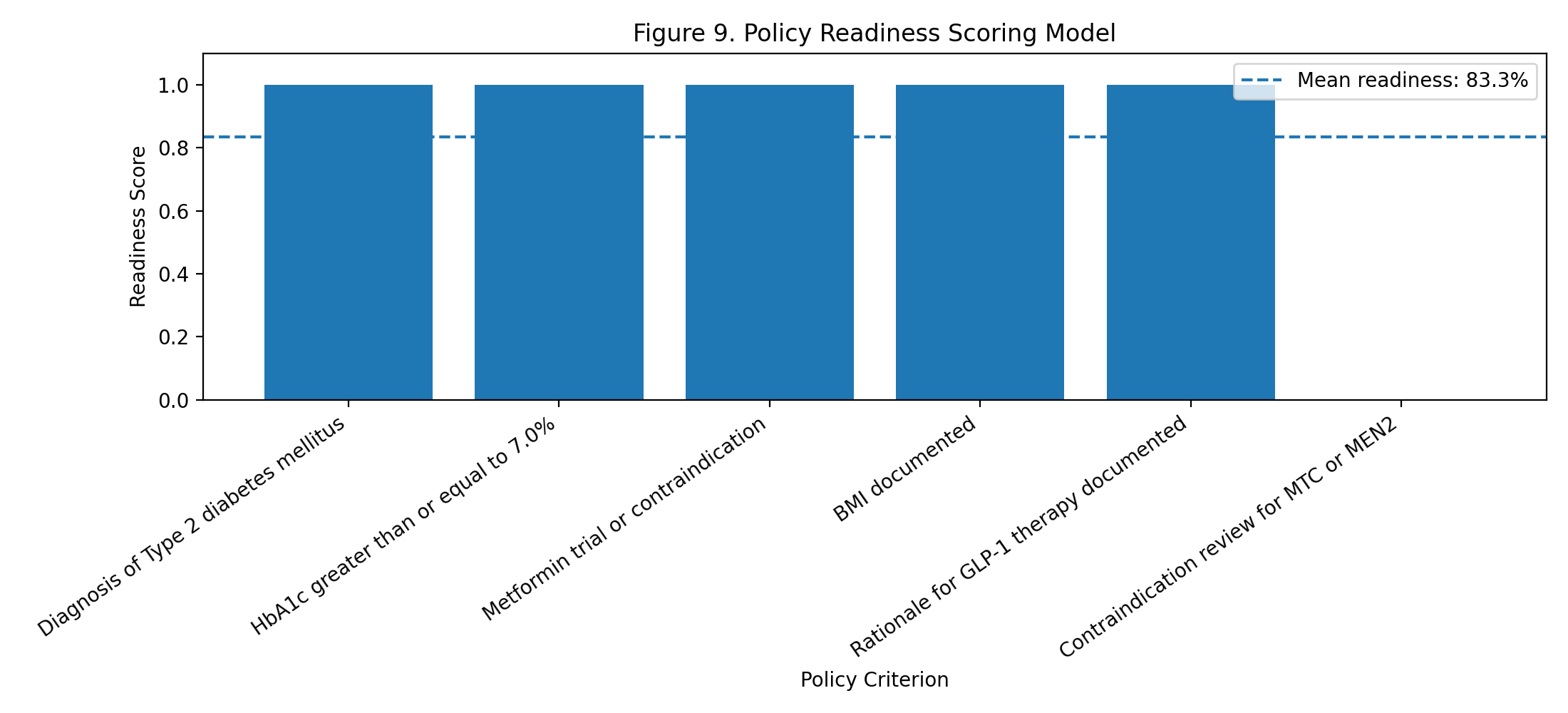
The readiness score assigns 1.0 to met criteria, 0.5 to criteria requiring review, and 0.0 to missing criteria. In the prototype, five criteria were met and one was missing:
7. Safety Gating Logic
The most important safety rule is that missing MTC/MEN2 documentation must not be interpreted as either an absent history or a positive history.
Unknown family history ≠ Positive family history
The correct representation is missing documentation requiring clinician confirmation.
8. Results
ClearPath matched five of six GLP-1 prior authorization criteria. The missing criterion was safety documentation for MTC/MEN2 family history. The final status was ready for clinician review with missing documentation.
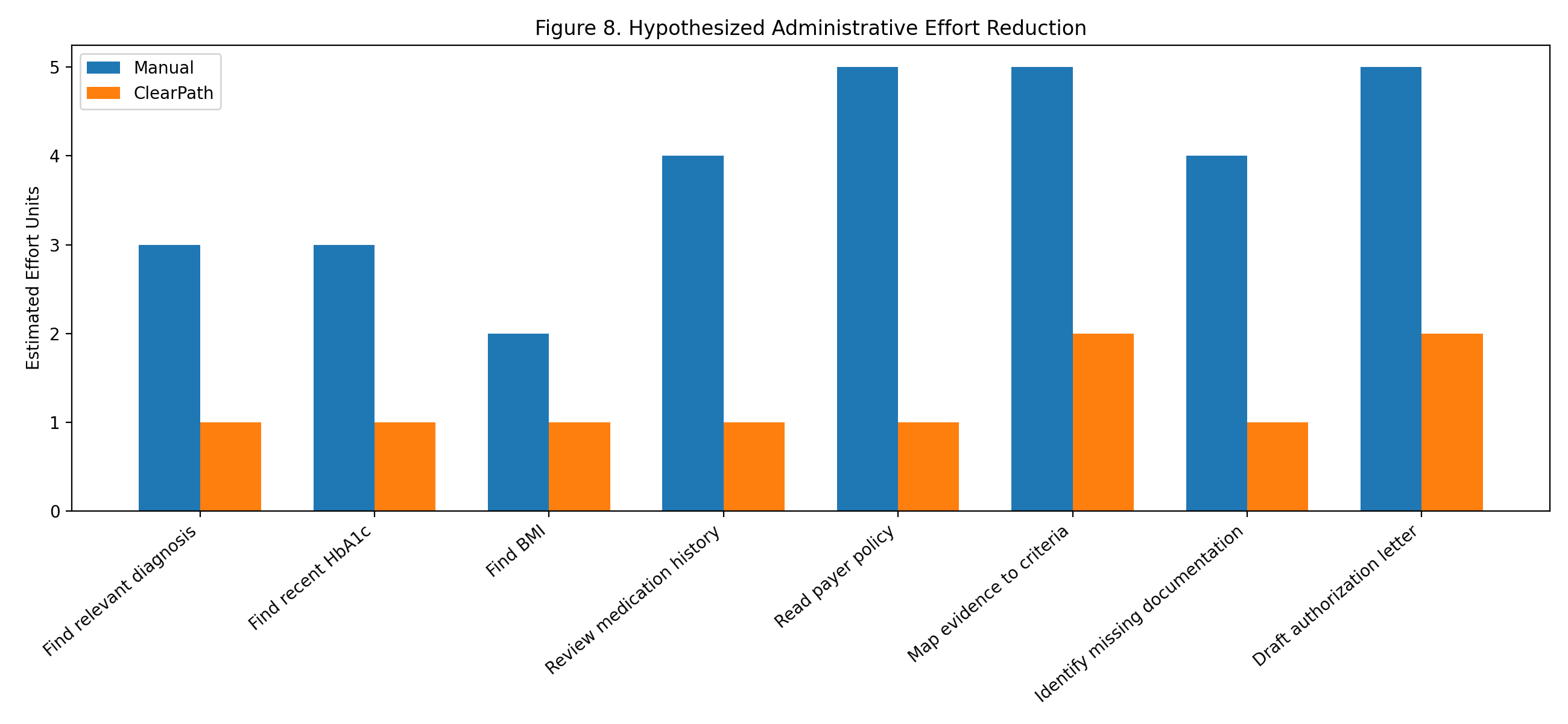
The hypothesized administrative effort estimate suggests that ClearPath could reduce evidence-gathering and packet preparation effort by approximately 67.7%, from 31 estimated manual effort units to 10 ClearPath-assisted effort units. This is a hypothesis-generating estimate rather than a measured time-motion study.
9. Discussion
ClearPath demonstrates that a Prompt Opinion agent workflow can transform patient facts and policy requirements into a structured prior authorization readiness packet. The system’s most important behavior is not that it writes a letter. The most important behavior is that it identifies missing safety documentation and refuses to overstate readiness.
Prior authorization is better understood as an evidence-alignment task. A complete packet requires alignment among patient facts, policy requirements, and safety constraints. ClearPath operationalizes this alignment while preserving clinician authority.
10. Limitations
This prototype uses a synthetic patient case and simplified GLP-1 policy criteria. The effort-reduction estimates are hypothesized, not measured. The live A2A policy-agent path encountered latency limitations, so the stable demonstration used a concise ClearPath prompt with policy criteria included directly. A production version should connect evidence extraction directly to live FHIR queries through MCP tools.
11. Future Work
Future work includes a production MCP server, stronger A2A orchestration, audit trails with evidence provenance, and expansion to additional prior authorization categories such as MRI, specialty referral, durable medical equipment, and high-cost biologic therapies.
12. Conclusion
ClearPath demonstrates a safe, interoperable, and clinically realistic approach to healthcare agent workflows. In the synthetic case, it identified five criteria as met and one safety criterion as missing, producing an 83.3% readiness score and the status ready for clinician review with missing documentation.
The project’s central contribution is not autonomous decision-making. Its contribution is safe administrative synthesis: converting fragmented context into a reviewable, standards-aligned deliverable.